The pandemic of diabetes mellitus represents a substantial global health challenge. Diabetes causes many long-term systemic complications that considerably impact the patient and society, as it typically affects individuals in their most productive years.(1) There are two types of diabetes, type 1 and 2. Type 1 diabetes mellitus (T1DM) is characterised by the destruction of beta cells in the pancreas by an autoimmune mechanism, whereas type 2 diabetes mellitus (T2DM) is a relationship between lifestyle and genetics.
The International Diabetes Federation published data that indicate that the prevalence of diabetes mellitus in Europe is 8.5% of people aged between 20 and 79 years, which means that 33 million people in the European Union are affected by this silent and severe condition.(2) The total number of people diagnosed with diabetes mellitus worldwide is projected to rise to 366 million in 2030.(3)
Diabetic retinopathy represents microvascular end-organ damage as a result of diabetes. The Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) Cohort showed that after 20 years of diabetes mellitus, 99% of patients with type 1 and 60% of patients with type 2 show some retinopathy.(4) Furthermore, a meta-analysis of 14 prospective studies showed that 1 in 4 with diabetes develop diabetic retinopathy within the mean follow-up period of 5.7 years, whilst another meta-analysis of 35 prospective studies revealed an incidence of DR among people with diabetes of 34.6%.(5,6)
There are established risk factors for developing diabetic retinopathy; diabetes duration, uncontrolled blood pressure and blood sugar levels, hypertension, dyslipidaemia, ethnicity, pregnancy, and smoking.(7) The role of glycated haemoglobin (HbA1c) in its correlation with the risk of developing and progressing diabetic retinopathy has been well established. The HbA1c is an important indicator of long-term glycemic control to reflect the cumulative glycemic history of the preceding two to three months.(8) There are two scales of HbA1c used in everyday clinical practice. The targets of diabetic patients under the old classification were between 6.5 and 7.5%, while the new measurement indicates 48-59 mmol/mol.(9) As per Diabetes Control and Complications Trial (DCCT), and later on confirmed by The Epidemiology of Diabetes Interventions and Complications Study (EDICS), the intensive control of blood glucose levels, where the mean HbA1c was 7.2%, achieved a decrease in the incidence of diabetic retinopathy by 76% and slowing the progression of diabetic retinopathy by 54%.(10,11)
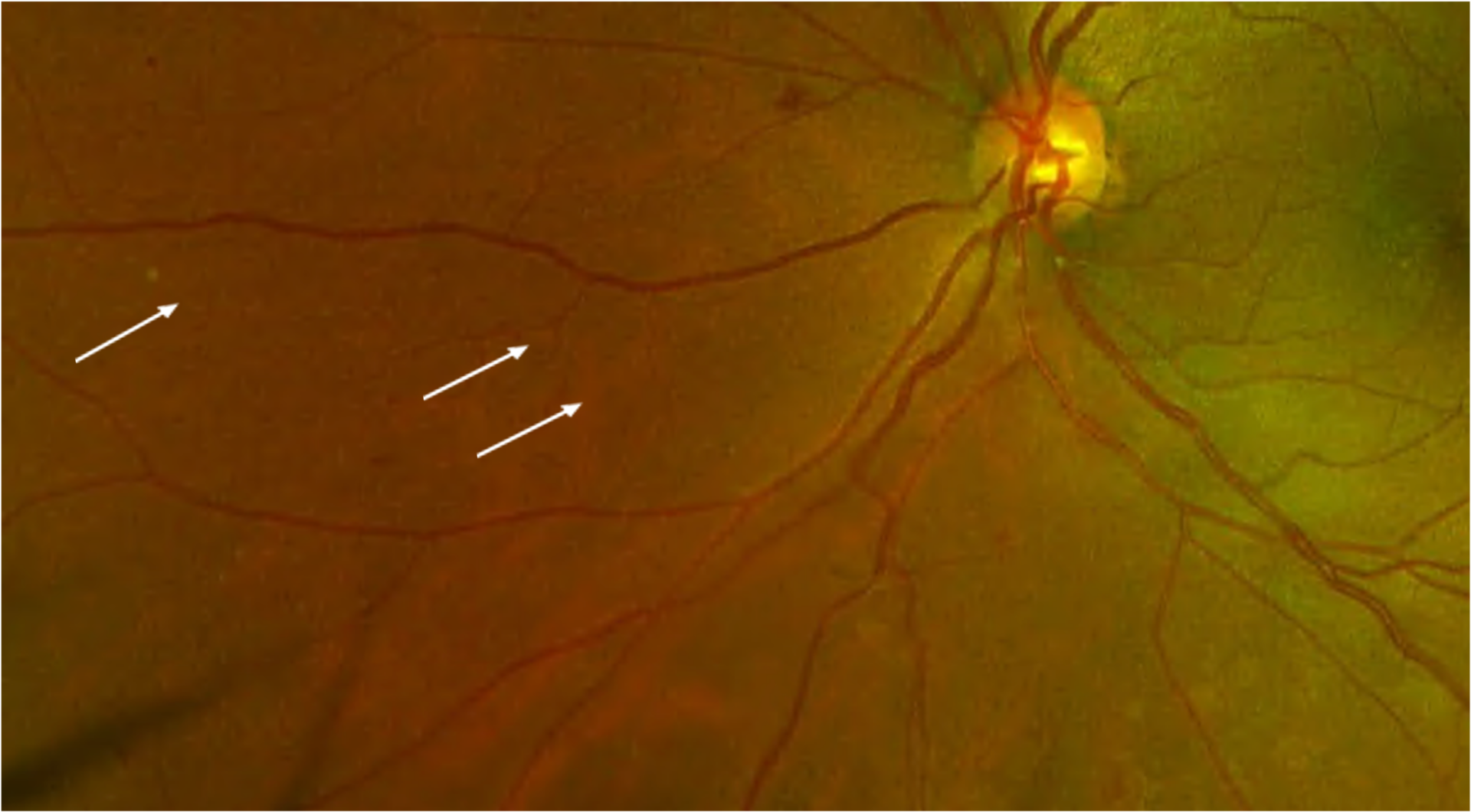
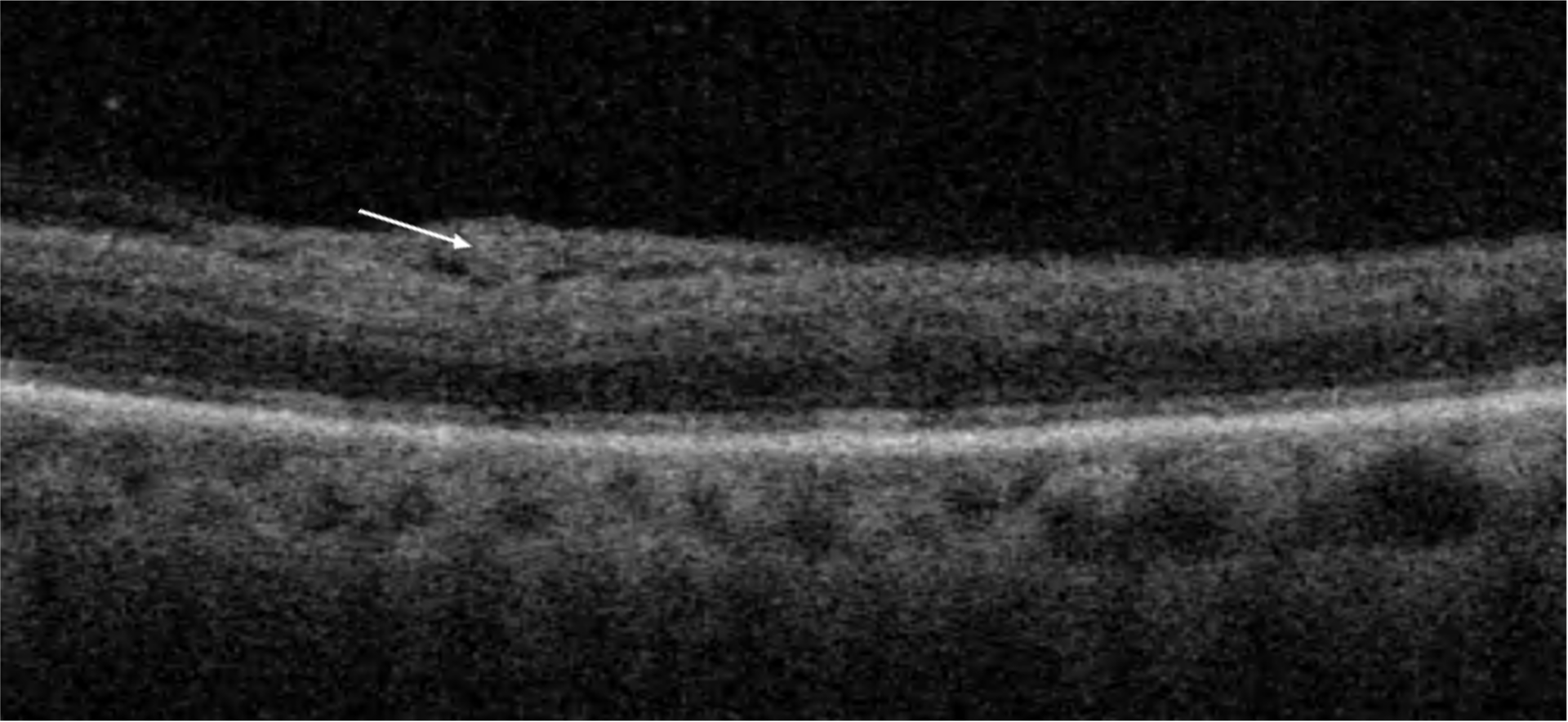
Diabetic retinopathy ranges from non-proliferative diabetic retinopathy (NPDR) and its stages to proliferative diabetic retinopathy (PDR). The proliferative stage is defined by the presence of new vessels of the retina, optic disc, and/or iris and iridocorneal angle. As the disease progresses, associated diabetic macular oedema may also become apparent. Three major events are involved in the pathomechanism of diabetic retinopathy and, consequently, in diabetic macular oedema; capillary leakage, capillary occlusion, and retinal ischaemia with its sequelae.(7) On the molecular level, hyperglycemia leads to the activation of alternative pathways of glucose metabolism, such as the polyol pathway, advanced glycation endproducts (AGEs) formation, protein kinase C (PKC) activation, hexosamine pathway flux, and Poly(ADP-ribose) polymerase activation.(12,13) The result of these pathways is the activation of cytokines and growth factors, leading to vascular endothelial dysfunction, increased vascular permeability, and eventual microvascular occlusion.(12) Microvascular occlusion leads to retinal ischemia, which promotes neovascularisation and the formation of IRMAs.(12)