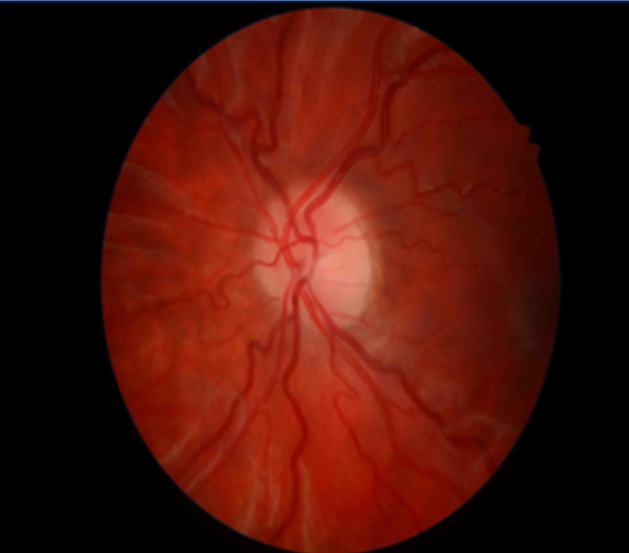
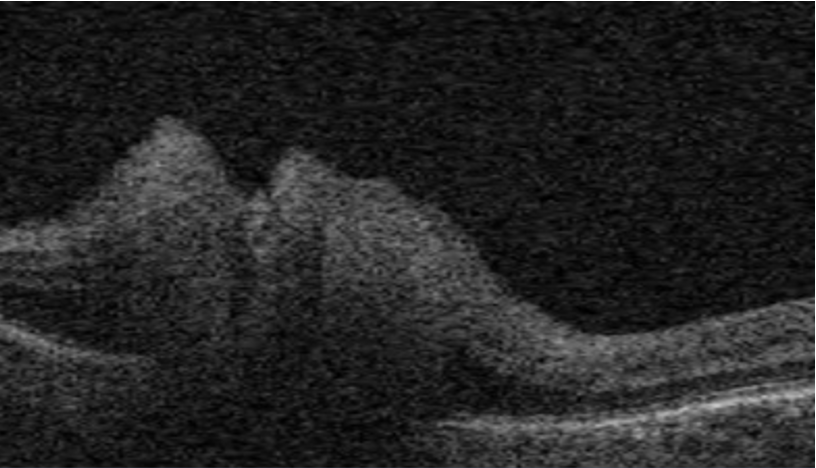
Papilloedema is a term that is exclusively used when disc swelling is secondary to increased intracranial pressure (ICP). (1) . We should distinguish papilloedema from optic disc swelling from other causes, which is named ”optic disc oedema”. As the papilloedema indicates increased intracranial pressure, it is an alarming sign. Potential causes of increased intracranial pressure are brain tumours, central nervous system inflammation (CNS), central venous thrombosis, and idiopathic intracranial hypertension.
It is essential to understand that optic disc oedema is a term used in all other causes when the optic disc swelling is not caused by increased intracranial pressure. For example, due to acute non-ischaemic optic disc neuropathy (NAION), inflammation of the optic disc, infiltration of the optic disc, etc.