Glaucoma represents a substantial public health problem. It is the leading cause of irreversible blindness worldwide and is associated with a reduced quality of life.(1)
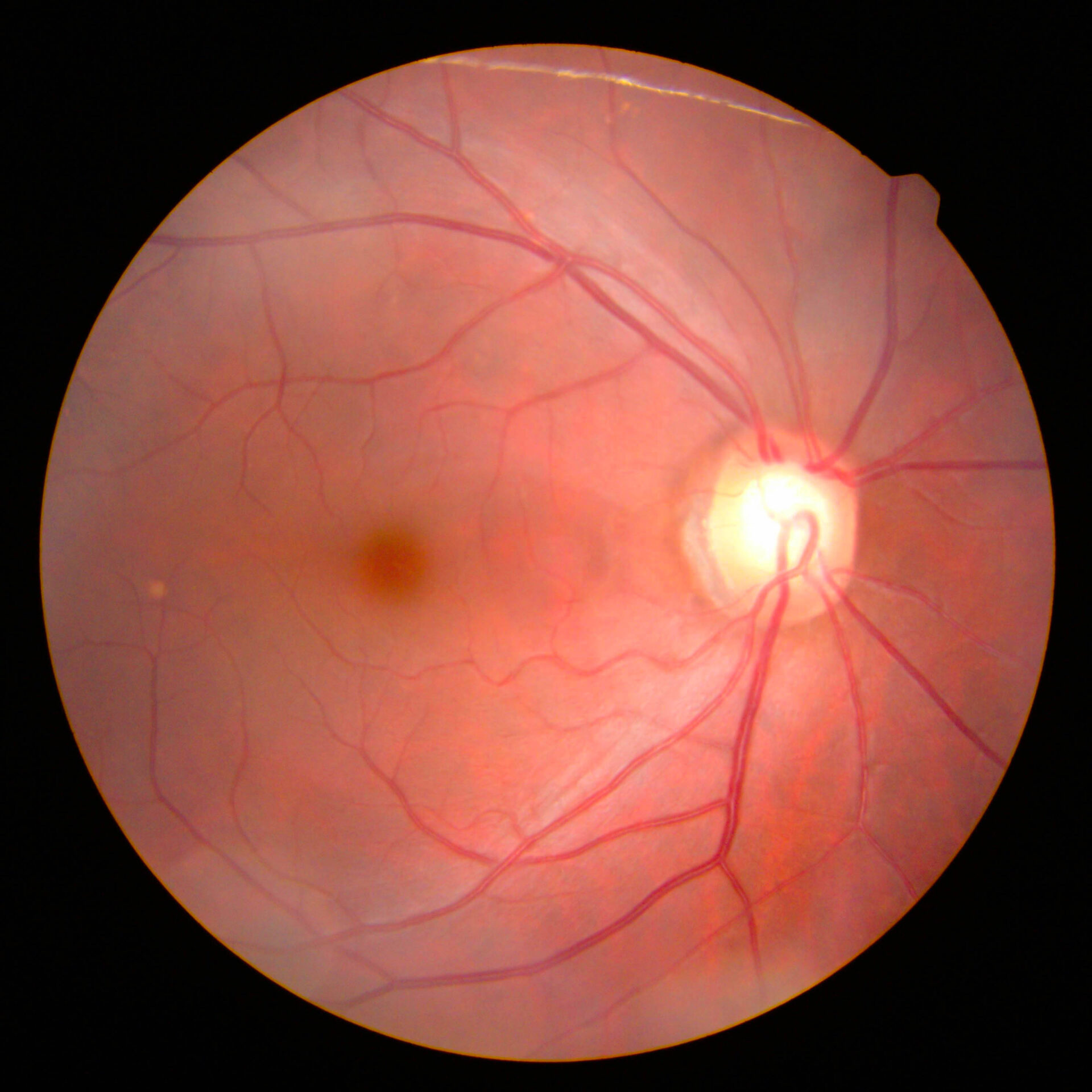
Glaucoma describes a group of progressive conditions with characteristic cupping of the optic disc with corresponding visual field defects due to retinal ganglion cell loss.(2)
In primary angle-closure glaucoma, the underlying mechanism is mainly pupillary block. At the same time, in secondary forms, there are other underlying causes that either push the iris forward from behind or pull the iris forward to contact trabecular meshwork.(3,4) Both angle-closure glaucomas may cause acute dramatic attacks or chronic asymptomatic disease. It is crucial to be familiar with the below terminology:(5)
- Primary angle-closure suspect (PACS) or narrow anatomic angle
- Primary angle-closure (PAC)
- Primary angle-closure glaucoma (PACG)
- Secondary angle-closure
Several risk factors are identified for primary angle-closure glaucoma: hyperopia, family history of angle closure, advanced age, female gender, Asian or Inuit descent, short axial length, shallow anterior chamber depth, and thick crystalline lens.(6-12)
A relative pupillary block causes primary angle-closure glaucoma in most cases. In the pupillary block, the aqueous humour encounters increased resistance to flow between posterior and anterior eye chambers. The increased pressure gradient across the pupil causes the peripheral iris to bow forward and cover some or all of the filtering portion of the trabecular meshwork, resulting in appositional angle closure. Peripheral anterior synechiae form after prolonged or repeated contact of the peripheral iris with trabecular meshwork.(3) Non-pupillary block mechanism is present in the plateau iris. A typical central anterior chamber depth, flat iris profile, and crowding of the angle by the iris base characterise plateau iris configuration. There is a forward displacement of the iris base by anteriorly located ciliary processes that can lead to subsequent angle closure.(13,14)
Mechanisms/causes of secondary angle-closure are absolute pupillary block due to 360º posterior synechiae, aqueous misdirection, swelling of the ciliary body in inflammatory conditions, choroidal swelling (i.e., choroidal detachment), scleral buckles, contracting membranes within the iridocorneal angle, iris incarceration in traumatic cases, iridocorneal endothelial syndrome.