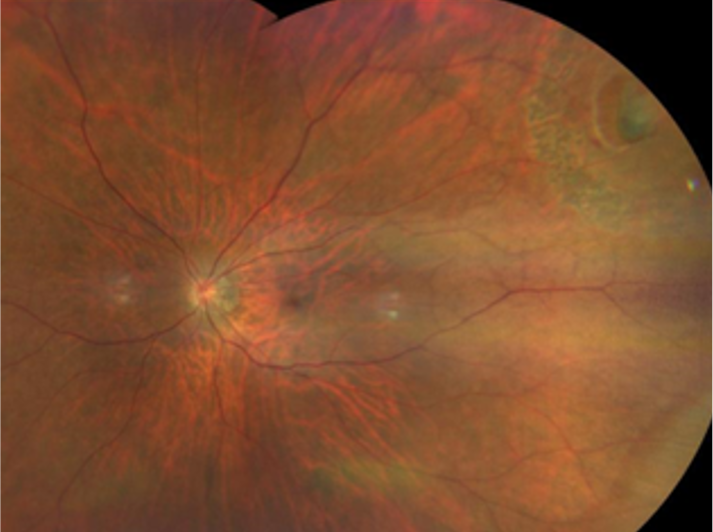
Retinal detachment is the separation of the neurosensory retina from the retinal pigment epithelium (RPE). It is a sight-threatening condition with an incidence of 1 in 10,000.(1,2) Furthermore, retinal detachment is more common in men, and mainly present in people between 40 and 70 years old.
Retinal detachment occurs when fluid accumulates in the virtual subretinal space. The classical categorisation of retinal detachment is rhegmatogenous, tractional, and exudative (serous). The rhegmatogenous retinal detachment (RRD) is the most common, and it occurs when there is a full-thickness retinal break secondary to vitreoretinal traction (most often during the process of posterior vitreous detachment (PVD)). The break allows fluid to enter the subretinal space and separates the neurosensory retina from the RPE.
Three elements need to be present for the rhegmatogenous retinal detachment:
- Abnormal mobility of partially liquefied vitreous.
- Tractional elements that cause retinal tear formation.
- Retinal break.
These are the risk factors for rhegmatogenous retinal detachment: lattice degeneration, peripheral retinal breaks, pathologic myopia, trauma, previous intraocular surgery, aphakia, family history, and previous retinal detachment. The peripheral retinal degenerations are important risk factors where lattice degeneration takes the primary position.(3)