Retinal detachment is the separation of the neurosensory retina from the retinal pigment epithelium (RPE). It occurs when fluid accumulates in the virtual subretinal space. The classic categorisation of retinal detachment is rhegmatogenous, tractional, and exudative (serous).(1)
The rhegmatogenous retinal detachment is the most common, and occurs when there is a full-thickness retinal break secondary to vitreoretinal traction (most often during the process of posterior vitreous detachment (PVD)). The break allows fluid to enter the subretinal space and separates the neurosensory retina from the RPE.(2-3)
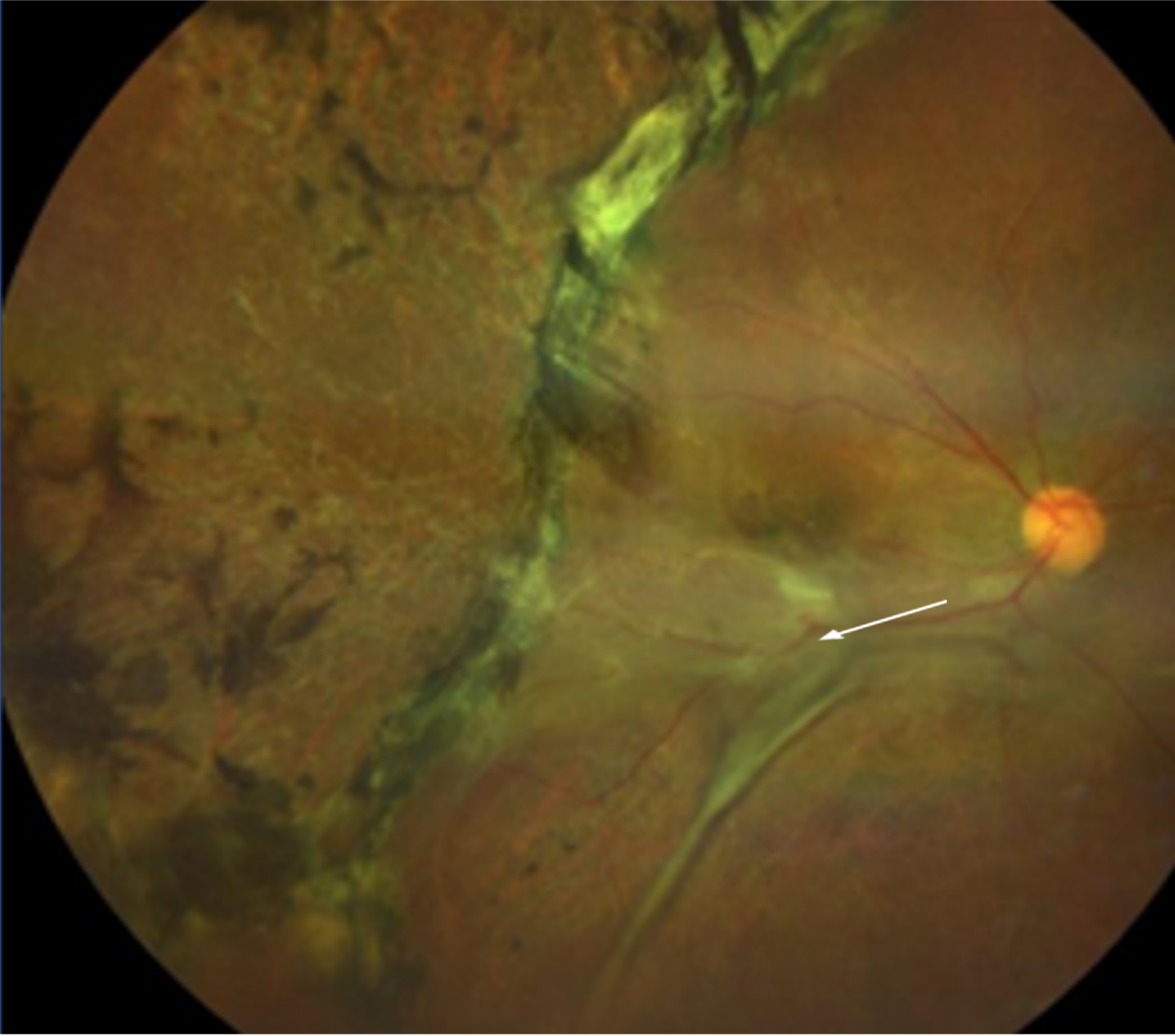
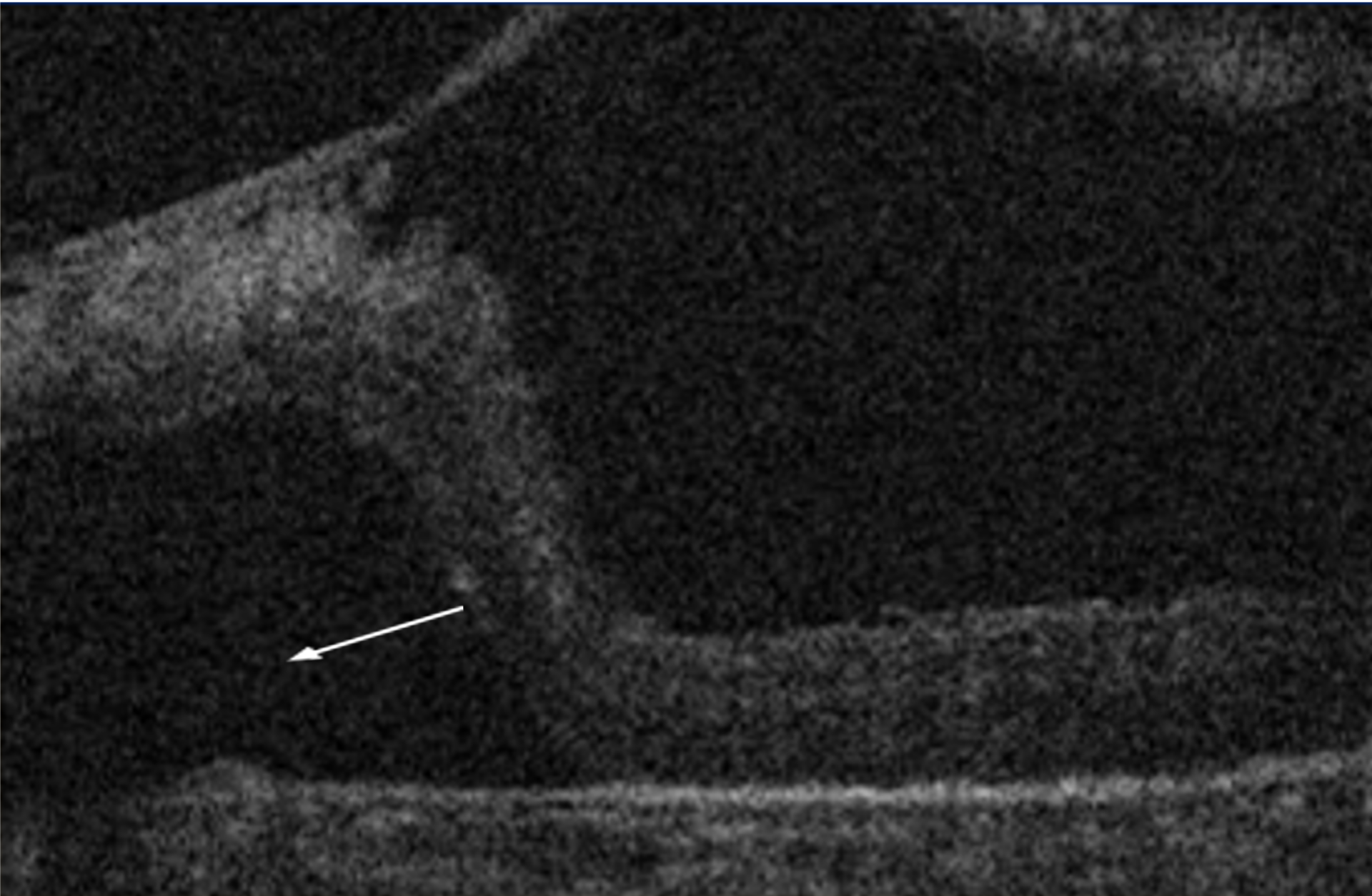
Tractional retinal detachment is the second-most common type of retinal detachment. The vitreoretinal forces mechanically pull the retina away from the underlying RPE. The tractional forces occur within the vitreous body or on the retinal surface. In most cases, there is the presence of a retinal surface membrane which is consisted of contractile cells like fibroblasts, RPE, and glial cells.(4) The tractional retinal detachment is seen in diabetic retinopathy, proliferative vitreoretinopathy (PVR), penetrating trauma, and retinopathy of prematurity (ROP).(5,6) Due to the mechanical pulling of the retina, the tractional retinal detachment has a concave appearance.
There are cases when a tear and traction combine, and such retinal detachments are called tractional-rhegmatogenous retinal detachments. This subtype is most commonly present in proliferative diabetic retinopathy, proliferative vitreoretinopathy, proliferative sickle cell retinopathy, and penetrating eye injuries.(7)
Retinal detachments can occur without a retinal break or vitreoretinal traction. These detachments result from a collection of subretinal fluid secondary to diseases of the choroid and RPE or of the retina itself.(1,7) In normal conditions, the retinal pigment epithelium actively pumps the subretinal fluid into the choroid, keeping the neurosensory retinal adherent. Various conditions lead to the failure of the RPE pump and cause exudative (mainly serous) retinal detachments.(2,8) Those conditions are primarily inflammatory or neoplasms: Vogt-Koyanagi-Harada disease, sympathetic ophthalmia, posterior scleritis, preeclampsia, severe and diffuse central serous retinopathy, malignant hypertension, malignant melanoma, choroidal haemangioma, and choroidal metastases.