Generally, legislation for optometry has more similarities than differences for the Northern European markets (the Nordic countries and the Netherlands). Some of the guidelines are old and, practically speaking, outdated. If a clinical guideline doesn’t meet the modern principles of person-centred care, it should most likely be reviewed.
Which tests to include – always
With that in mind, here are a few selected standard tests that are always useful to include in your routine eye examination.
Anamnesis
The most important activity in the entire test. You can’t skip it even for the slightest presenting problem. We must create an atmosphere with the patient that invites them to talk about the presenting problem and ask questions. Avoid questions that can be answered by yes or no. I’ve looked into several complaint cases in eye care over the years, and it’s surprising how many times a medical file doesn’t explain why the patient wanted the eye exam. I recommend adding a questionnaire before the patient sees you, to assist the anamnesis process. It’ll help you get structured information, and it’ll help the patient understand what information you need from them.
Visual acuity
Uncorrected visual acuity is under-evaluated, and we often forget to measure it. However, you should measure it every time a patient comes in because it indicates how they see without correction. It’s the baseline measure for how the patient experiences their dependency on glasses and contact lenses. Uncorrected visual acuity defines the size of the visual disability. Without understanding that, you can’t fully understand the patient’s need.
It’s amazing how much variability you can find in uncorrected visual acuity among persons with the same refractive error. I personally often refer to my good friend with -4,5D correction. She prefers to be uncorrected most of the day. She is an artist, a painter inspired by her own thoughts and visualisation, and she doesn’t care if her distance vision is a bit blurry when she works. Believe it or not, she has 0,4 in uncorrected VA without squeezing her eyelids.
Measuring visual acuity is a skill that needs practice in listening to both what and how the patients express themselves. Some patients need more time, and others are fast. The speed of the test can also indicate what the underlying problem is. Think of keratoconus, cataracts, and early macular conditions. It can be tricky for the patient to give feedback on visual acuity in these situations because of reduced contrast or metamorphopsias, right?
While ophthalmologists are trained to use a pinhole when examining subjects with reduced visual acuity or when having difficulties refracting a patient and achieving the expected acuity, I find that optometrists usually don’t perform this test. Yet, it’s both easy and fast. Therefore, I’d claim that a referral about reduced visual acuity, where pinhole visual acuity is missing, is incomplete.
Refraction
A “no-brainer”. Note that modern refraction technologies are so good that you can skip the cross-cylinder method in many cases. To explain how to do that without reducing refraction quality is out of scope for this text. A good start is to read the user guide for your autorefraction device if one of the most modern ones.
To be good at refraction, you need to have an indication of the patient’s maximum pupil diameter when it’s dark. Without knowing the diameter, you can’t estimate the effect of the refractive shift that an eventual huge pupil can induce. Modern autorefractors will measure this automatically if you do the test in reduced light conditions.
Remember that young patients, and not only children, can benefit from refraction in cycloplegia.
When giving feedback about referral quality from optometrists, ophthalmologists often mention that they prefer to get them from us instead of the GP’s because we are more precise and have refraction and VA.
Binocular testing
This text doesn’t cover which tests to perform when there are symptoms or indications of binocular problems. As I see it, every vision exam should include the test below, even if there are no symptoms of binocular vision:
- Cover test at a distance and near
- Convergence near point
- Motility by pen torch
These three are fast to perform and give a lot of relevant information for the choice of products on how to correct refractive errors.
Eye health
Eye health is tricky to define as optometrists need an extensive battery of tests to evaluate our patient’s eye health. The list below is what I consider the minimum set of tests. Add other tests if you suspect diseases. Again, it’s about the right tools for the right problem, but you should perform a core of tests every time:
- Structured capturing of risk factors for eye conditions
- Pupillary testing using a pen torch
- Visual field screening for new patients – can be confrontation testing like Donders
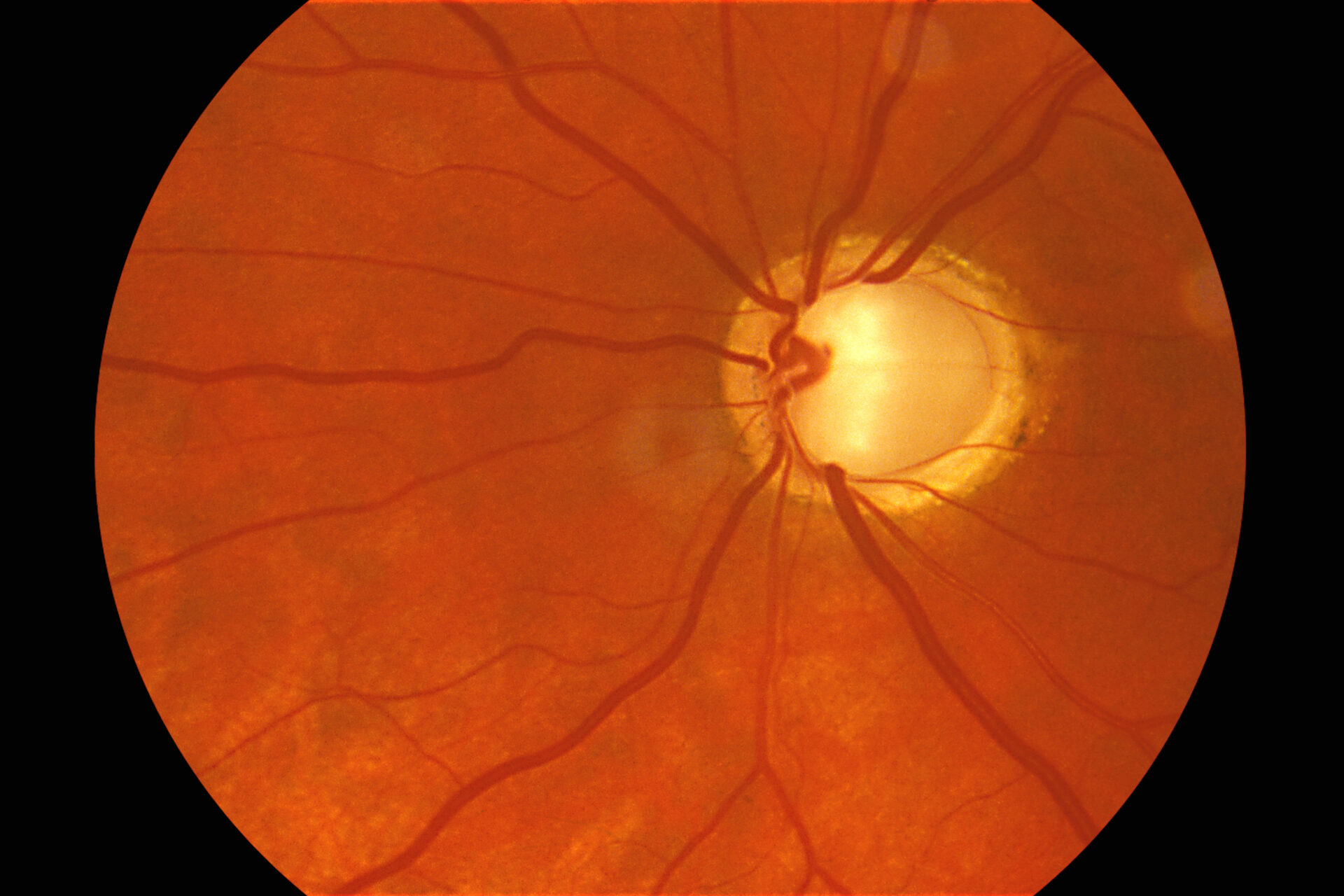
- Visual inspection of the eye front to back by images and screening by slit lamp
Remember that when you see a finding on eye images, you’ll need to examine it in 3D. Using a +90 or similar together with a slit lamp is the gold standard. Yes, OCT gives 3D images, which is good and, in some cases, better than manual use of +90. Still, colours and shadings are not the same as with +90. OCT is black and white (or with artificial colours). Fundus cameras that use laser scanning show you artificial colours as well. You need to know all errors in the technology you are using to know precisely what you are doing.
Which tests can be delegated?
What tasks you can delegate varies in every country. You might find a discrepancy between what national and general laws say about delegating tasks in healthcare versus what national optometry regulations say. Again, make sure what is valid for your market. If there is reason to disagree, the optometry organisations should pick it up. Remember that WHO is clear that more delegated work is needed in healthcare.
The practical impact on delegations within optometry can – and will – be diverse because of different national market regulations. However, below are some areas for your reflection.
Can we delegate:
- Mapping of symptoms and risk factors for eye diseases?
- Performing subjective best refractions and visual acuity?
- Imaging the eye?
- Informing about correction options?
- Taking care of contact lens handling and fitting, if an optometrist supervises it?
To move forward in delegating tasks, we need a good reason to do it. As I see, the primary reasons are a lack of optometrists and more effective use of resources. Delegating more will mean that optometrists can let go of some repetitive tasks, making it more attractive to be an optometrist.
Conclusion
Remember that you must rely on evidence-based methods when using a problem-orientated approach. It means you should choose the right tests for the right problem. Always consult the national and association optometry guidelines but don’t let them decide which tests to perform. Instead, you should select the tests based on a case-to-case basis. However, a standard set of tests helps detect certain diseases or developments such as glaucoma at an early stage – even if the patient currently has no apparent symptoms. A time-efficient eye examination balances these basic tests and tests targeted at the presenting symptoms.