- CSCR typically occurs in males in their 20s – 50s, who exhibit acute or sub-acute central vision loss or distortion. Other common complaints include micropsia, metamorphosis, hyperopic (most common) or myopic shift, central scotoma, and reduced contrast sensitivity and colour saturation.
- The pathophysiology is not fully understood, but CSCR is thought to occur due to hyperpermeable choroidal capillaries and dysfunction of the retinal pigment epithelium dysfunction. The imbalance in the amount of fluid that enters the subretinal space and the ability to remove it results in a net accumulation of fluid beneath the retina, causing a serous detachment of the neurosensory retina. (See image 3)
- It is associated with stress and the use of prednisolone (both for oral use, skin and ocular).
- Most patients will spontaneously recover visual acuity within six months (average recovery time 3 to 4 months). Some patients may have some residual symptoms, such as distortion, decreased colour and contrast sensitivity, as well as visual difficulty at night.
- Despite an overall good prognosis, 40 to 50% of patients experience one or more recurrences in a 10-year time frame.

Sep 22, 2021
Chapter 6: Macular diseases
Introduction
Written by
Viewpoint
This chapter covers the following common macular diseases:
- Central serous chorioretinopathy
- Early age-related macular degeneration
- Late age-related macular degeneration
Click on one of the cards below to read more about the specific eye condition.
Chapters
Chapters
01
Central serous chorioretinopathy
01
Central serous chorioretinopathy
Referral: Normal depending on impact*
Central serous chorioretinopathy (CSCR) is the fourth most common retinopathy after age-related macular degeneration, diabetic retinopathy and branch retinal vein occlusion.

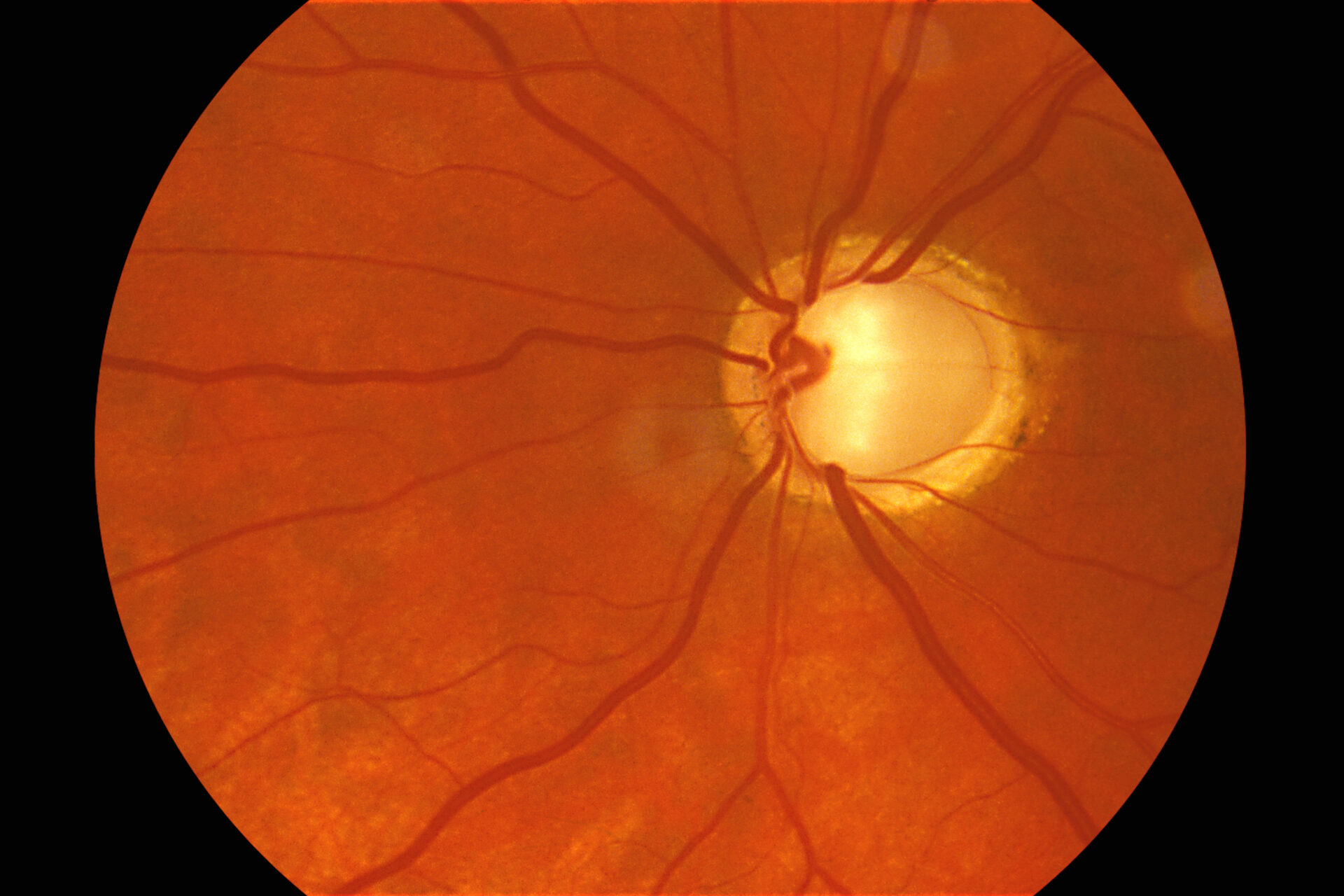
Image 1: Recurrent central serous choroidopathy
This image was originally published in the Retina Image Bank. Edwin H. Ryan, MD VitreoRetinal Surgery, PA. Retina Image Bank. Year 2012; Image Number 246. © the American Society of Retina Specialists.

Image 3: Recurrent central serous choroidopathy
This image was originally published in the Retina Image Bank. Edwin H. Ryan, MD VitreoRetinal Surgery, PA. Retina Image Bank. Year 2012; Image Number 245. © the American Society of Retina Specialists.02
Early age-related macular degeneration
Referral: Depending on patient characteristics*
Age-related macular degeneration (AMD) is an acquired degeneration of the retina that causes significant central visual impairment.
- Dry AMD (early form) is the most common form of the disease, affecting ~ 90 % of the patients.
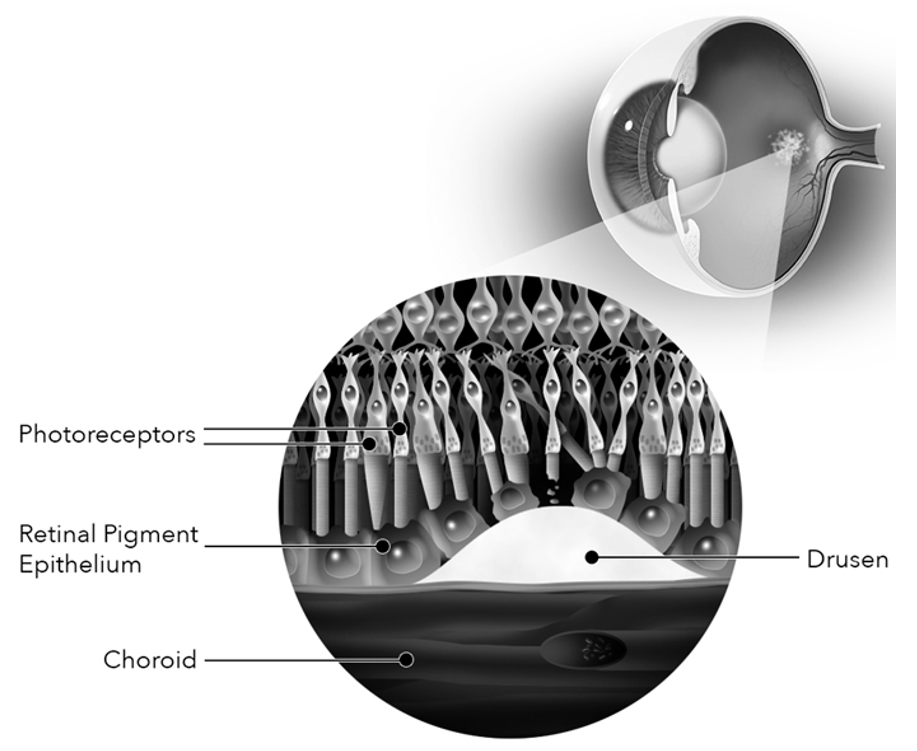
- The early form of the disease is characterized by the presence of drusen, subretinal pigment epithelial deposits located between the basement membrane of the retinal pigment epithelium (RPE) and Bruch’s membrane, or within the Bruch’s membrane itself. (See image 5)
- Other typical features of dry AMD include RPE disturbances such as granularity and atrophy of the RPE.
- Drusens vary in size and characteristics.
- Soft indistinct drusen and pigment abnormalities are considered high-risk characteristics for the development of later stages of the disease, geographic atrophy or neovascular AMD. (See image 7)
- There is no effective treatment for dry AMD. However, antioxidant and mineral supplementation has been shown to reduce the risk of progression in AMD.

Image 4: Image showing dry AMD with central drusen
Courtesy of Zeiss: Roger A. Goldberg, M.D. Bay Area Retina Associates

03
Late age-related macular degeneration
Referral: Depends on wet or dry, if wet soon*
The advanced form of AMD can be classified into the neovascular (exudative) and non-neovascular (nonexudative) forms.
- A typical non-neovascular manifestation of an advanced stage of dry AMD is geographic atrophy. It can be defined as a sharply delineated area of hyperpigmentation.
- Geographic atrophy involves degeneration of retinal pigment epithelium (RPE) cells that tend to create an island of lost photoreceptors, related to visible underlying choroidal vessels. (See image 8)
- The neovascular form of late AMD is characterized by the presence of choroidal neovascularization.
- Choroidal neovascularization indicates the abnormal growth of new choroidal vessels into the subretinal space above and beneath the RPE.
- Fundus imaging analysis may show a more or less visible greenish-grey subretinal lesion. (See image 9)
- Other signs, related to the growth of abnormal vasculature, can be sub-macular fluid, haemorrhages, and lipid exudation.
- Optical coherence tomography and anti-vascular endothelial growth factor (VEGF) therapy together have revolutionized the treatment of exudative AMD. Ranibizumab (Lucentis, Genentech, San Francisco, CA), Bevacizumab (Avastin, Genentech, San Francisco, CA), and Aflibercept (Eylea, Regeneron Pharmaceuticals Inc., Tarrytown, NY), are frequently used in the treatment of exudative AMD.



*Referral advice
The referral advice in the atlas should be used as a general guideline. The Optometry Atlas does not establish a standard of optometric care and specific outcomes are not guaranteed. Please read the full details here.