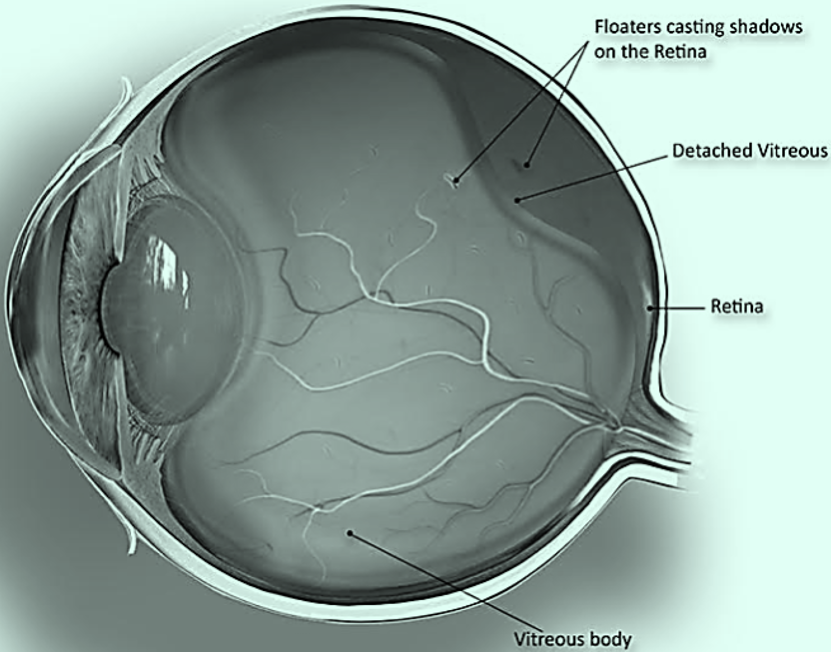
- There are millions of fine fibres intertwined within the vitreous that are attached to the surface of the retina.
- As we age, the vitreous gel slowly shrinks and these fine fibres pull on the retinal surface.
- Usually, the fibres break, allowing the vitreous to separate and shrink from the retina. This is a common condition that usually affects people over age 50, and is very common after age 70.
- In most cases, vitreous detachment is not sight-threatening and requires no treatment.
- As the vitreous shrinks, it becomes somewhat stringy, and the strands may cast tiny shadows on the retina noticed as floaters. Floaters may be accompanied by flashes of light (or lightning streaks) in peripheral vision.
- But if patients have new onset of symptoms with flashes or floaters, they should always have a dilated fundus examination from a practitioner with suitable training and experience. Always warn the patient of the risk of retinal detachment.

Sep 22, 2021
Chapter 2: Vitreous
Introduction
Written by
Viewpoint
The vitreous is the largest structure in the eye, and although it contains very few cells, some vitreous-related conditions can occur. This chapter covers the following:
- Posterior vitreous detachment
- Asteroid hyalosis
- Vitreous haemorrhage
Click on one of the cards below to read more about the specific eye condition.
Chapters
Chapters
01
Posterior vitreous detachment
01
Posterior vitreous detachment
Referral: Urgent to normal depending if retina involved and signs/symptoms*
Most of the eye’s central cavity is filled with vitreous, a gel-like substance that helps to maintain the eye’s round shape. Vitreous is 99% water, the remaining 1% is made up of collagen and hyaluronic acid giving it a gelatinous consistency and optical clarity.

02
Asteroid hyalosis
Referral: Refer if causing visual problems*
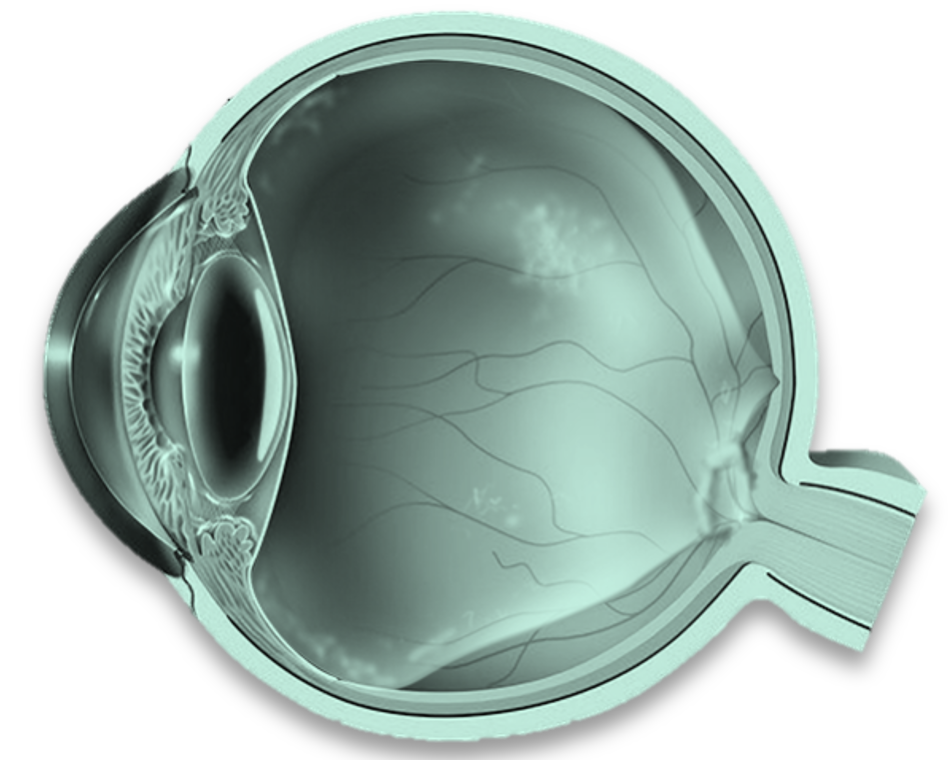
Minute white opacities composed of calcium-containing phospholipids are found in otherwise normal vitreous.
- Asteroid hyalosis has an overall incidence of 1 in 200 people, most frequently in those over 50 years of age.
- The condition is unilateral in 75% of the cases, and it only rarely causes any significant decrease in visual acuity.
- Clinical studies have confirmed a relationship between asteroid hyalosis and diabetes and hypertension.
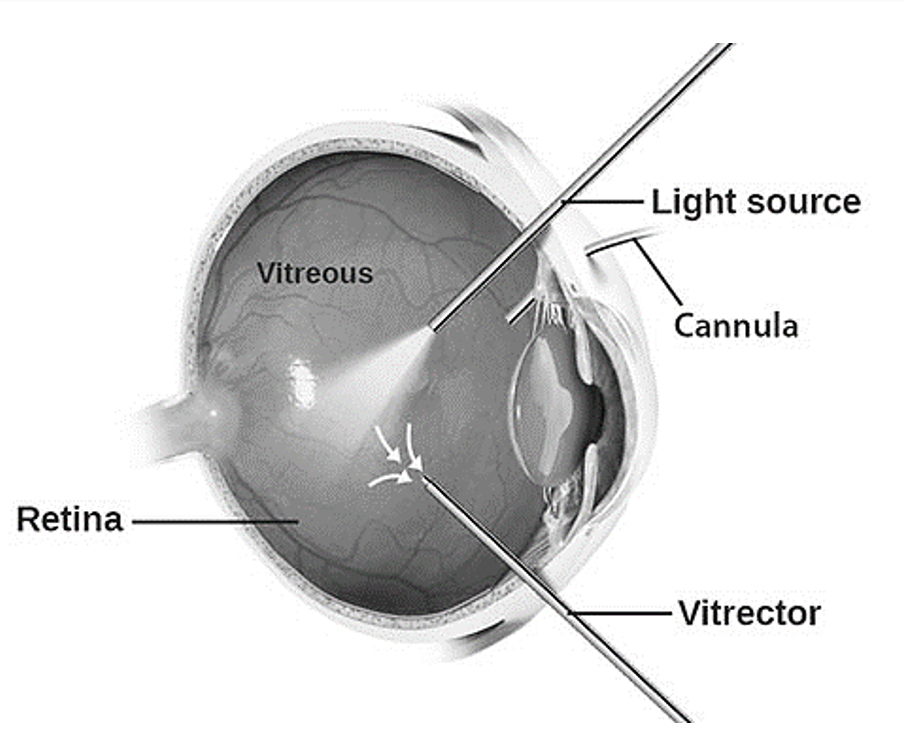
- Occasionally, vitrectomy may be necessary to remove visually significant opacities or to facilitate treatment of underlying retinal abnormalities such as proliferative retinopathy or choroidal neovascularization.
- Differential diagnosis: Synchysis scintillans, that is accumulated cholesterol particles. It is associated with the e.g. advanced stages of diabetic retinopathy, chronic uveitis and chronic vitreous haemorrhage.


03
Vitreous haemorrhage
Referral: Urgent*
The vitreous space represents 80% of the eye and has a volume of ~ 4 ml.
- The vitreous is firmly attached to the retina in three places:
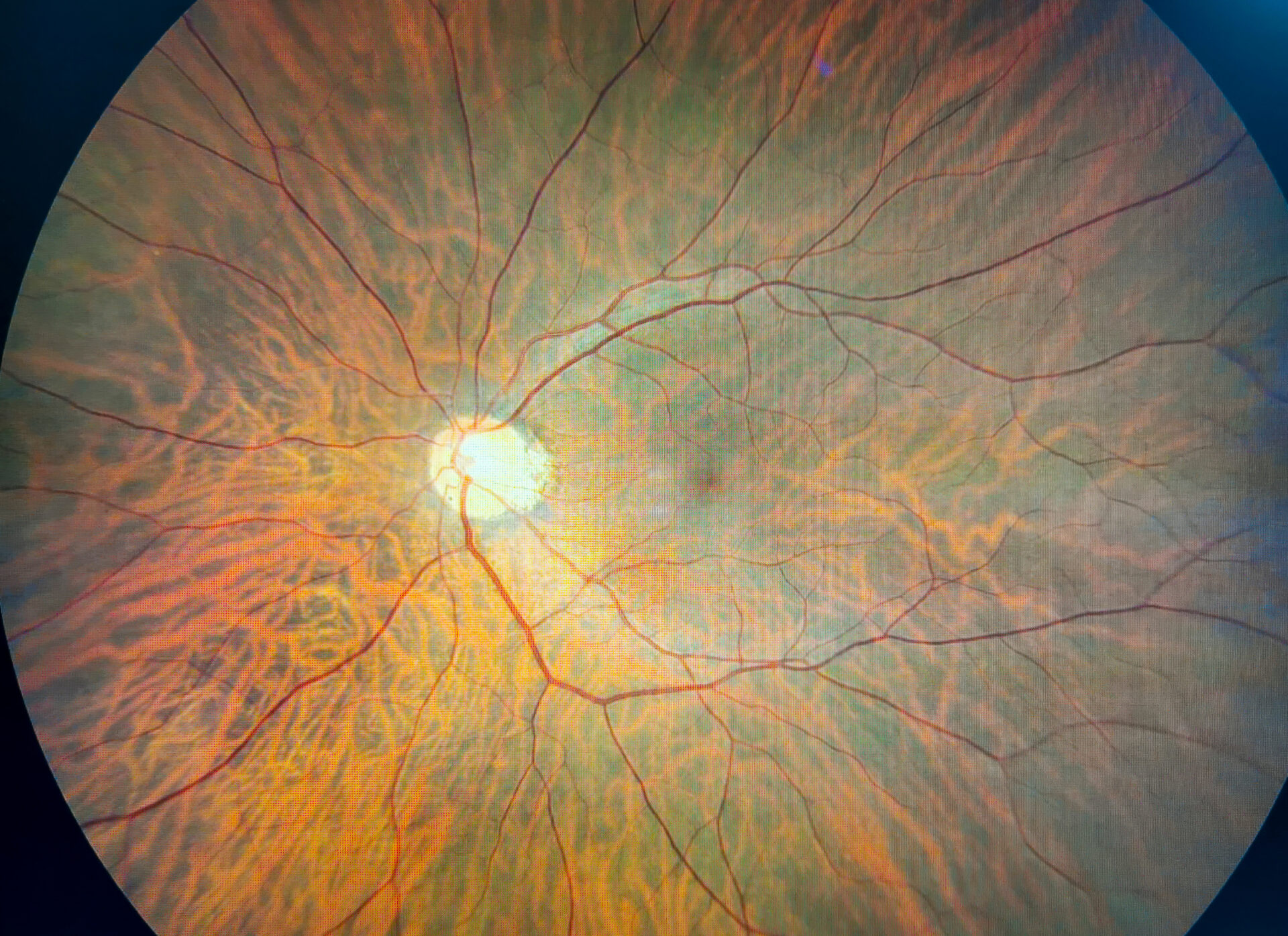
- the strongest attachment is anteriorly at the vitreous base (see image 8)
- followed by the optic nerve head, and
- retinal vasculature
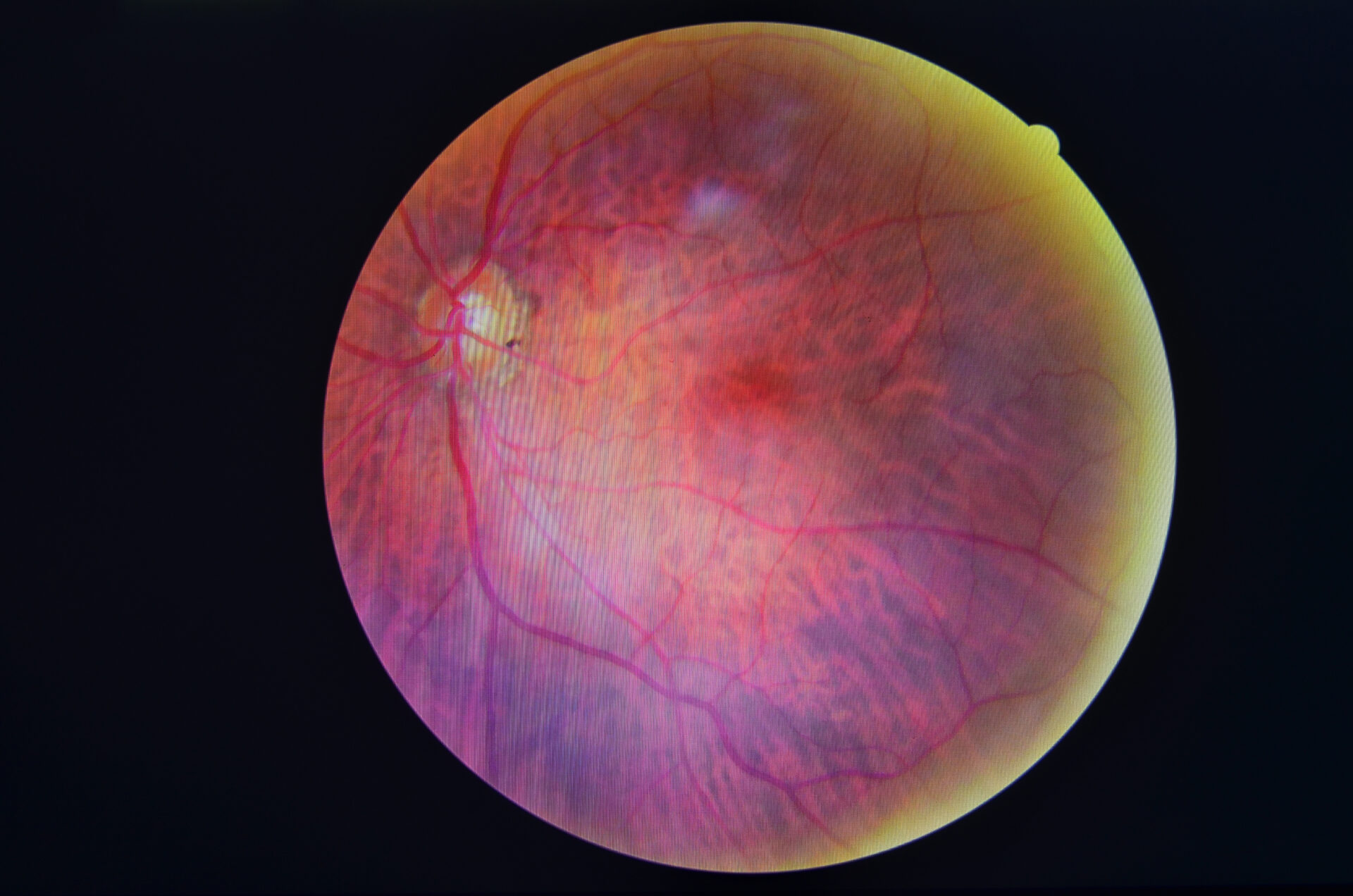
- Normal vessels can rupture when sufficient mechanical force overcomes the structural integrity of the vessel wall.
- During a posterior vitreous detachment, vitreous traction on the retinal vasculature may compromise blood vessels, especially at the firm attachments. (See image 9)
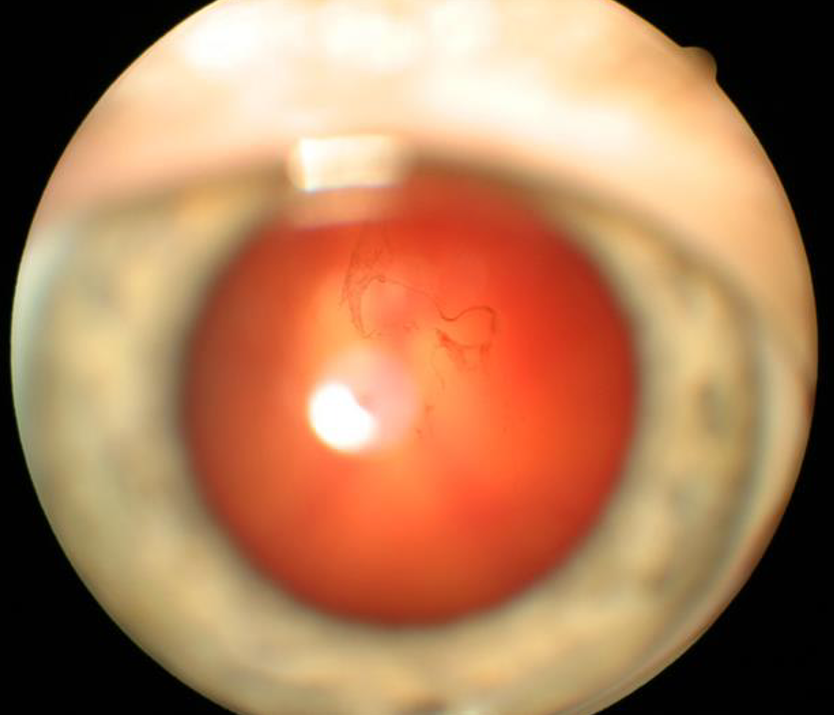
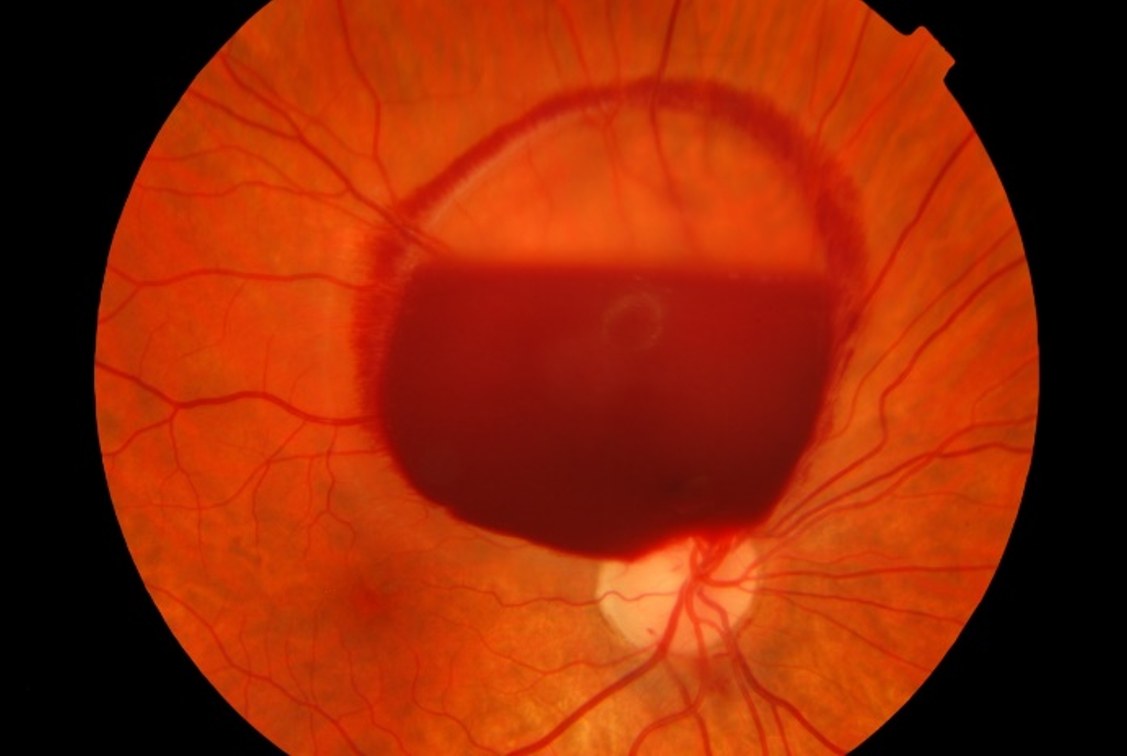
- The symptoms of vitreous haemorrhage alternate, but usually include painless unilateral floaters and/or visual loss.
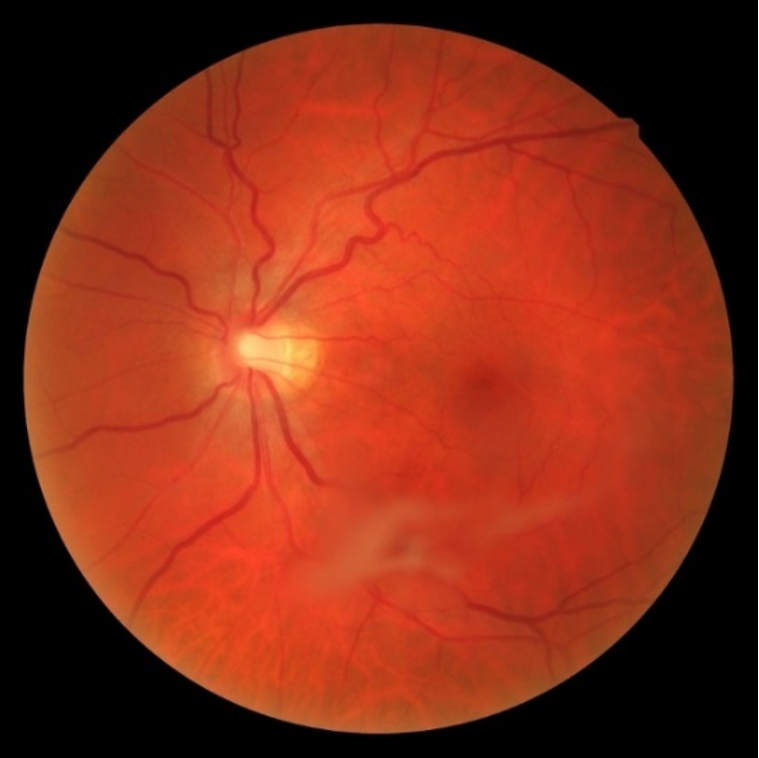
- Mild haemorrhage may be described as floaters, cobwebs, haze, shadows or red hue. More significant haemorrhage limits visual acuity and visual fields or can cause scotomas. (See image 10)

Patient case video: vitreous haemorrhage from retinal tear caused by posterior vitreous detachment | Randall Wong, Retina Eye Specialist
*Referral advice
The referral advice in the atlas should be used as a general guideline. The Optometry Atlas does not establish a standard of optometric care and specific outcomes are not guaranteed. Please read the full details here.